Are we as church called to care for orphans? You bet. Are we expected to use the gifts and talents entrusted to us to support families who respond to such a noble calling? They should expect nothing less!

November is Caregiver Awareness Month. As someone who became one of my dad’s caregivers before I started school, I grew up thinking everyone in the world was aware of caregivers and caregiving. As a young adult my husband and I cared for a son born with a life-threatening medical condition, and his typical sibling. As members of the sandwich generation, my brother, sister, and I cared for our mother for 15 years after she was diagnosed with dementia. This explains why, when I first heard that November is Caregiver Awareness Month, I was incredulous, and I still am.
In this episode, Lauren Hickman shares her personal journey and calling to disability ministry, describing how God has guided her every step of the way to serve families impacted by disability.
In today’s episode, Sandra talks about the challenges small to normative-sized churches face in disability ministry and shares how the churches she’s been a part of have overcome these challenges.
This week Elaina, from Key Ministry, sits down with Sergei Marchenko, Lead Pastor of Chatham Bible Church, and Special Needs Parent. They discuss preparing for the holiday season, church inclusion, special needs parenting and more!
The potential effects of trauma and abuse on the developing brain and nervous system are powerful and incredibly complex.
Healthy brain development is highly contingent upon a number of highly interrelated neuroregulatory systems that are highly sensitive to the effects of environment and experience. In some instances, environmental factors influence the expression of genes responsible for proteins affecting neurotransmitter sensitivity and function. In other instances, circulating hormones affect development of critical brain regions associated with learning, memory, impulse control, mood and emotional self-regulation.
The neuroregulatory systems that help us to manage stress throughout life are extremely malleable during the prenatal period and early childhood. Toxic levels of stress during this period affect the development of these neuroregulatory systems in ways that cause those systems to become overly responsive to shut down in response to a wide range of stressors in later life.
Let’s look at how toxic stress affects the development of different systems and structures in the brain…
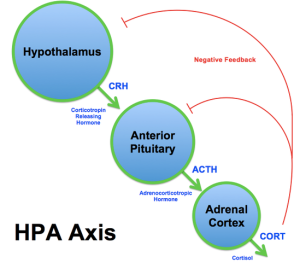
The hypothalamic-pituitary axis (HPA): The HPA plays a critical role in the body’s response to stress. The hypothalamus produces corticotropin-releasing hormone (CRH) which stimulates the pituitary gland to produce adrenocorticotropic hormone (ACTH). ACTH acts on the adrenal gland to increase levels of cortisol (see diagram at top of page). Cortisol is a steroid hormone produced in response to a wide variety of stressors. Cortisol mobilizes energy stores and suppresses immune response. Surgeons prefer to operate early in the morning when cortisol levels tend to be at their highest. Long-term elevation of cortisol levels in children (as seen in kids exposed to high levels of acute or chronic stress/abuse) can turn off the glucocorticoid receptor gene (involved with regulation of the long-term stress response of the brain to cortisol) and the myelin basic protein gene, producing the “insulation” of nerve cells that allows for efficient nerve signal transmission. Elevated cortisol levels also cause damage to the hippocampus (below).
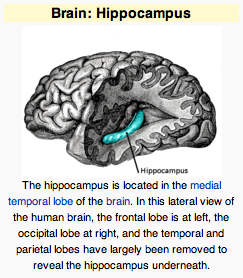
The hippocampus: The hippocampus is a structure that plays a key role in learning by consolidating information from short-term to long-term memory. The hippocampus is capable of growing new neurons in adulthood. Damage to the hippocampus from elevated cortisol levels in childhood leads to impairments in learning and memory.
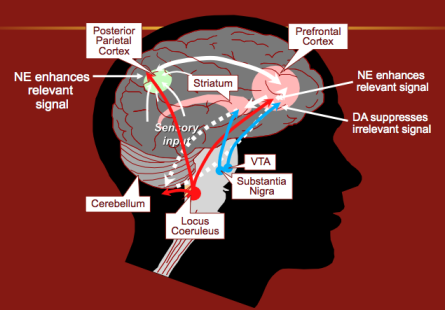
The locus coeruleus/noradrenergic brain systems: The locus coeruleus is a region located in the brainstem where the cell bodies of most noradrenergic neurons are located. This system is involved with regulating the overall level of arousal in the central nervous system. Exposure to stress/trauma early in life have been associated with lifelong increases in noradrenergic reactivity.
The noradrenergic system (along with the dopaminergic system) is the primary system associated with executive functioning. Tracts of neurons originating in the locus coeruleus project to the posterior attention center in the parietal cortex (responsible for scanning the environment for relevant stimuli) and the anterior fronto-striatal system, which is more involved with executive control and focusing attention. The posterior center is primarily under noradrenergic control, while the anterior center receives both dopaminergic and noradrenergic projections. Difficulties associated with weaknesses in executive functioning include poor impulse control, diminished capacity for emotional self-regulation, delaying gratification and problems with working memory. Editor’s note: This may help to explain the increased prevalence of ADHD among kids who have been traumatized or abused along with the observation they are frequently less responsive to medication than kids with ADHD lacking such exposure.
Dopaminergic systems: Numbing, decreased interest in pleasurable activities and difficulties with ability to maintain focus upon a task are associated with pathways mediated by dopamine. Dopamine pathways originating in the midbrain projecting to the medial prefrontal cortex may be especially vulnerable to the effects of acute and chronic stress. These pathways also play a role in selective information processing, working memory, and applying previously learned information to new experiences. Pathways from the medial prefrontal cortex to the amygdala are thought to play a role in mediating the response to fear.
Serotonergic/GABA systems: Alterations in these systems in response to stress/trauma contribute to difficultiess in social attachment and regulation of mood and affect following early stress.
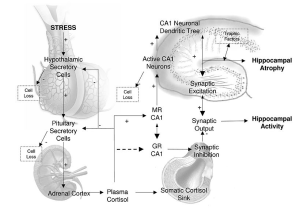
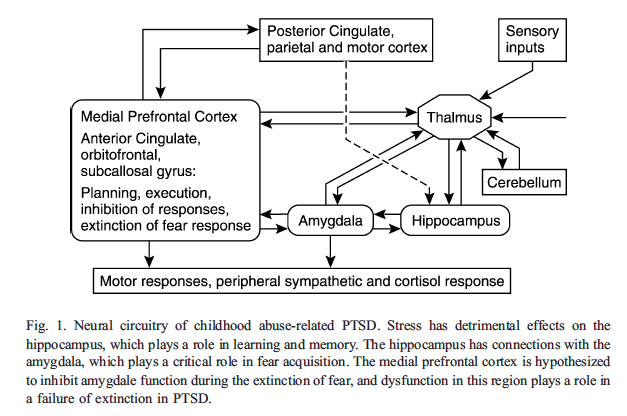
Here’s a diagram from an article in Child and Adolescent Psychiatric Clinics of North America that shows the interrelationship of the different neural circuits involved in childhood PTSD…
Bottom line…The neuroendocrine changes that occur in response to trauma in children are widespread, long-lasting, and impact mood, learning, arousal, impulse control, memory, emotional self-regulation, and contribute greatly to future response to stress.
Updated March 4, 2016
We’ll take a closer look in this post at the new companion diagnosis to Reactive Attachment Disorder related to pathologic care in early childhood… Disinhibited Social Engagement Disorder.
Studies of children who have been maltreated or raised in institutions have demonstrated two characteristic patterns of emotional response and behavior in response to pathologic caregiving environments. The first pattern involves emotional withdrawal…kids who lacked a preferred attachment figure, failed to respond to comfort when distressed, demonstrated decreased social and emotional reciprocity, decreased positive affect and unexplained fearfulness or irritability. Their symptoms could be described as internalized. This is the group we discussed in a previous post who will continue to be described as meeting criteria for Reactive Attachment Disorder (RAD). In contrast, the second group was observed to demonstrate indiscriminately social behavior-inappropriately approaching unfamiliar adults and a lack of concern for strangers… in some instances, a willingness to wander away with strangers. They may also exhibit a lack of ability to maintain an appropriate sense of body space, and may also demonstrate disinhibition of behavior.
Research has demonstrated that these two patterns differ in terms of clinical correlates, course, and response to treatment. There was also much greater interrater reliability among clinicians using diagnostic criteria based upon the assumption that the two patterns represented separate and distinct conditions compared to the existing DSM-IV criteria for Reactive Attachment Disorder. As a result, the authors of the DSM-5 chose to establish a separate diagnosis of Disinhibited Social Engagement Disorder (DSED) to distinguish the second group from children with Reactive Attachment Disorder. This new designation corresponds to the condition in the ICD-10 referred to as Disinhibited Attachment Disorder of Childhood. Disinhibited Social Engagement Disorder encompasses the vast majority of children and teens we’ve treated in our practice who in the past were identified with attachment disorders.
Here are the criteria for Disinhibited Social Engagement Disorder in the DSM-5:
A. A pattern of behavior in which a child actively approaches and interacts with unfamiliar adults and exhibits at least two of the following:
B. The behaviors in Criterion A are not limited to impulsivity (as in Attention-Deficit/Hyperactivity Disorder) but include socially disinhibited behavior.
C. The child has exhibited a pattern of extremes of insufficient care as evidenced by at least one of the following:
D. The care in Criterion C is presumed to be responsible for the disturbed behavior in Criterion A (e.g., the disturbances in Criterion A began following the pathogenic care in Criterion C).
E. The child has a developmental age of at least nine months.
Specify if Persistent: The disorder has been present for more than 12 months.
Specify current severity: Disinhibited Social Engagement Disorder is specified as severe when a child exhibits all symptoms of the disorder, with each symptom manifesting at relatively high levels.
First, we’ll start by looking at the similarities between kids with DSED and RAD. Both conditions are linked to social deprivation, neglect and pathologic care, and are readily identified among children being raised in institutional settings. Both conditions appear to be relatively stable over time in institutionalized children. But some very key differences exist as well…
We can anticipate lots of confusion because the vast majority of children presenting for clinical care will meet the diagnostic criteria for DSED as opposed to RAD, since DSED is more likely to persist after kids leave pathologic care and causes more difficulties with interpersonal relationships. DSED is easier to observe across settings, especially in schools. I can certainly understand why the name of the condition was changed…not all kids with DSED lack attachments…but I’m not sure this distinction will be recognized by a majority of clinicians for quite some time.
Updated March 1, 2016
There are many reasons why children adopted from orphanages and children in foster care frequently exhibit severe problems with conduct and emotional self-regulation. Effects of trauma and neglect upon brain development combined with genetic and environmental influences appear to be responsible in most instances…as opposed to a primary attachment disorder.