0
items
$0

FDA takes action on "bad" versions of generic Concerta
Editor’s Notes: The FDA announced plans to rescind the approval of generic versions of Concerta manufactured by Kremers Urban Pharmaceuticals and Mallinckrodt Pharmaceuticals. The drug companies have until mid-November to file a request for a hearing to appeal the decision. Thanks to all of our readers who contacted the FDA to share their experiences with these products.
Below is our original post explaining why the two most recent versions of generic Concerta are less effective than the original product and the generic version sold by Actavis Pharmaceuticals...
I’d ask our regular blog readers to allow me to digress today while I share about a medication issue that is greatly impacting many of the kids and families we serve.
Concerta is the most commonly prescribed medication to teens in the United States. When the product first hit the market in 2000, it revolutionized the treatment of ADHD because Concerta offered the first truly effective method for prolonging the effects of methylphenidate (the active ingredient in Ritalin and many other stimulant preparations) so that kids no longer needed to go to the principal’s office or nurses’ office in the middle of the school day. When Adderall XR followed in 2001 and Strattera in 2002, a vast increase ensued in the number of children and teens identified with and treated for ADHD. Out of the roughly 25 medications approved for ADHD, Concerta remained very popular because of the consistency of its’ effects throughout the school day into the time immediately following school. It is widely used in teenagers because of its’ beneficial effects on driving performance.
A basic principle in understanding how extended-release stimulant products work is that the manner in which the drug is released into the body (the drug delivery system) has profound effects on the pharmacodynamics (the observed benefits/response to the drug). We have quite a number of approved medications for ADHD in which methylphenidate is the active ingredient. In addition to Concerta, Ritalin LA, Metadate CD, Daytrana, Quillivant and Focalin XR are all extended-release methylphenidate products. The effects of the medication at specific times throughout the day result from the differences in how the medication is released and absorbed into the body with each unique delivery system, and form the basis of how we decide which product we choose for an individual child. Allow me to illustrate…
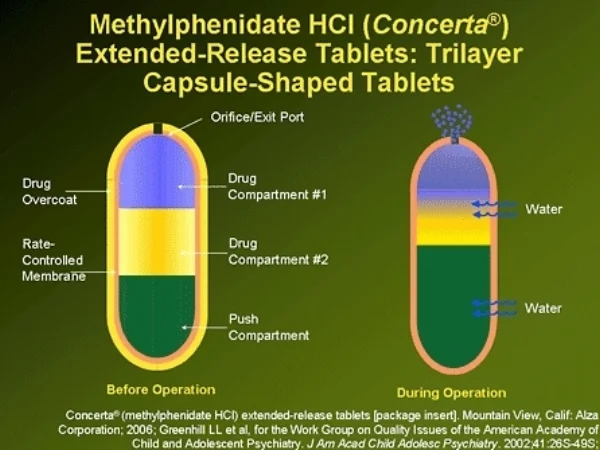
Concerta utilizes something called the OROS delivery system (see featured picture at the top of this blog post) to release methylphenidate into the body. It was developed by a team of scientists in California who observed a phenomena referred to as “tachyphylaxis” with earlier attempts to develop long-acting methylphenidate-based stimulants. Essentially, people taking stimulants develop some degree of tolerance to the drug acutely in response to an individual dose. While the absolute level of the drug in someone’s system matters, whether the blood level is rising or falling also matters, since a rising blood level contributes to the ability of a stimulant to sustain beneficial effects over the course of a school or work day.
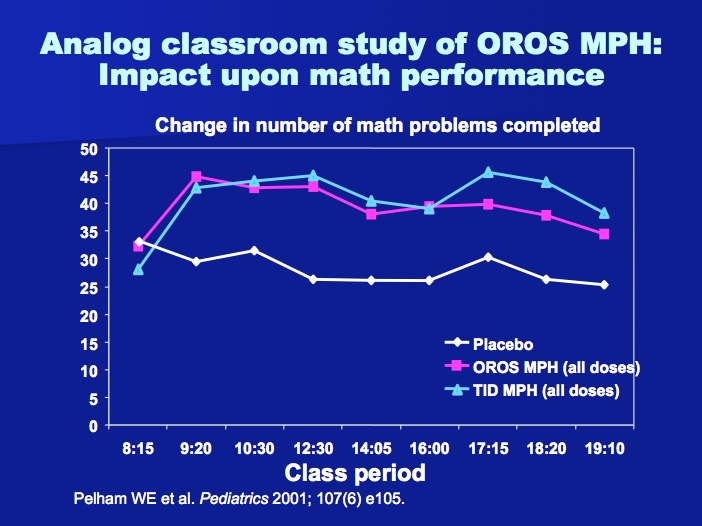
Concerta was designed to release an initial dose of stimulant within the first two hours of ingestion…22% of the active drug is contained within the coating of the pill. After this overcoat dissolves, a laser-drilled hole in the end of pill is uncovered. As the pill passes through the stomach and the gastrointestinal track, water taken up into the pill results in changes in internal pressure that leads to a “pulse release” of small amounts of medication as it passes through the gut. The effects of Concerta were tested in a laboratory classroom setting, in which raters blinded to whether kids received active drug or placebo scored the observable behavior of kids throughout a twelve hour day, and an age-appropriate mini-math test (PERMP) was administered at intervals throughout the day to measure the effects of medication on cognitive performance. The results are pictured below. A significant benefit of Concerta is the consistency of improvement in cognitive performance throughout the day.
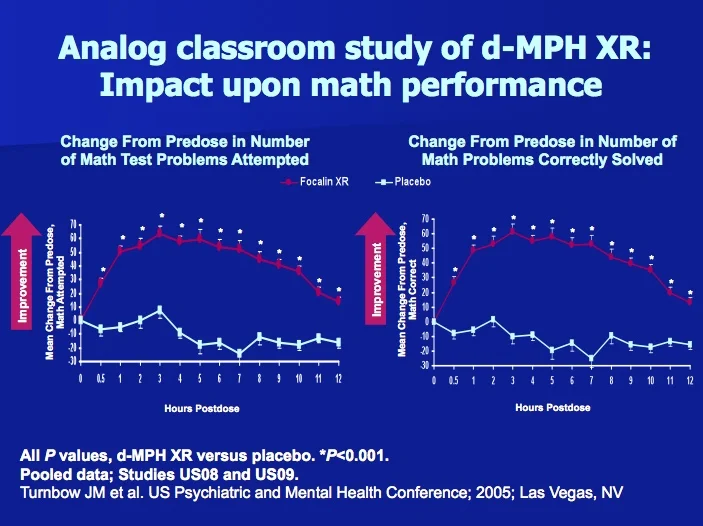
In contrast, Focalin XR utilizes a “beaded” delivery system to release methylphenidate into the body. Focalin XR is a capsule containing two types of beads. The outer coating of the capsule dissolves very quickly (within ten minutes) upon ingestion. 50% of the beads inside Focalin XR release almost immediately after the coating of the outer capsule dissolve, while another 50% have a different coating designed to dissolve approximately four hours after the capsule is swallowed. One advantage of Focalin XR is that parents can crack open the capsule and sprinkle the contents in yogurt or applesauce when kids can’t swallow pills, whereas Concerta won’t work if the pill isn’t swallowed intact. Another advantage with 50% of the medication released immediately is that the medication kicks in very quickly in the morning with demonstrable benefits at 30 minutes (see below). In practice, Focalin XR has a pronounced peak effect in late morning and is very effective for most kids throughout the school day. At the same time, the cognitive effects of the drug fall off much more quickly during the latter part of the day compared to Concerta, and drug company marketing claims aside, I find in my patients that Focalin XR is a good choice for kids who need medication to cover the duration of their school day, but not much longer.
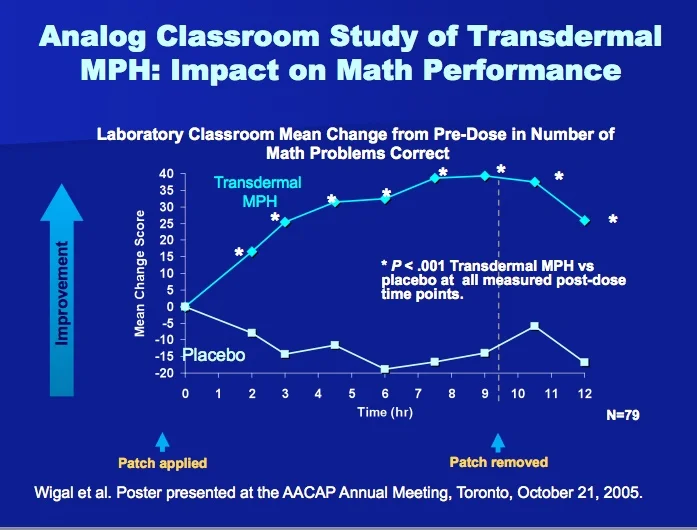
Daytrana is a patch worn on the hip in which methylphenidate is absorbed through the skin as a result of an osmotic gradient…the difference in the concentration of methylphenidate in the patch vs. the difference in the concentration of methylphenidate in the capillaries supplying blood to the skin. A unique benefit of Daytrana is that it will last longer than any of the other stimulant products on the market…it was originally developed to be a 16-18 hour drug. Because the testing required for approval by the FDA examined the effects of the product over a twelve hour period, the company that manufactures Daytrana isn’t permitted to share that information with prescribers. The cognitive effects of Daytrana also peak later in the day than with other products (see below), making Daytrana very helpful for many kids who struggle with homework after school. Comparing the laboratory classroom studies of Daytrana to Concerta and Focalin XR, an obvious downside to Daytrana is that it doesn’t work as well during the first half of the school day. Many parents resort to either putting the patch on their child very early in the morning while they’re still sleeping to overcome this effect, or give their child a small dose of immediate-release methylphenidate (Ritalin or immediate-release Focalin) when they first put the patch on in the morning.
My point is that what makes Concerta work like Concerta is the OROS delivery system. The same drug (methylphenidate) released through a different delivery system produces a VERY different response.
The arrival of generic Concerta was delayed for a number of reasons…the makers of Concerta fought the lawsuits of the generic manufacturers aggressively, and pursued a legal strategy involving what’s referred to as a “Citizen’s Petition” requiring generic companies seeking to copy Concerta to demonstrate a similar pattern of ascending blood levels throughout the day. Because Johnson & Johnson (the parent company that owned the rights to Concerta) owned the patent on the OROS release system, companies seeking to make a generic version had to do so with a different delivery system.
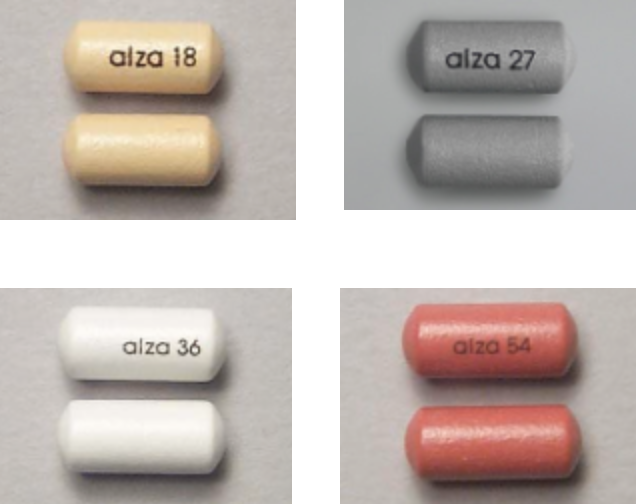
Ultimately, Watson Pharmaceuticals (subsequently acquired by Actavis) was approved to manufacture a generic equivalent of Concerta. As often occurs in these situations, the lawyers for Johnson & Johnson and Watson worked out a deal to avoid years of legal battles in which J & J would continue to manufacture Concerta through their Alza subsidiary that Watson would sell at a discount as an “authorized generic,” with the two companies splitting the profits. The brand Concerta and the Activis version of Concerta are equivalent…they are manufactured in the same factory, using the same equipment and the same drug delivery system as in the original Concerta. Pictures of the “authorized generic” using the OROS system are shown below:
The last two versions of versions of generic Concerta (manufactured by Mallinkcrodt and by Kremers Urban) each use very different drug delivery systems (release mechanisms) in an effort to replicate the therapeutic effect of Concerta.
In the case of the Mallinkcrodt product (pictured below), an overcoat containing immediate-release methylphenidate that dissolves within the first hour after ingestion. The core of the pill contains a diffusion-controlling membrane that releases methylphenidate as water in the gastrointestinal tract passes through the membrane. The membrane is designed to release methylphenidate over a period of time roughly corresponding to the release period resulting from the OROS delivery system in Concerta.
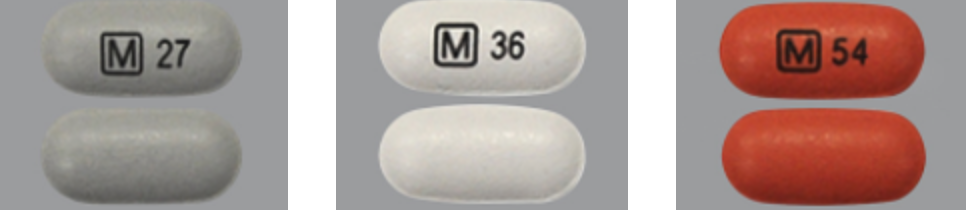
The Kremers Urban generic (pictured at right) uses an extended-release bead technology to release methylphenidate at a controlled rate. The pill resembles a conventional tablet in appearance, featuring an overcoat containing immediate release stimulant that releases during the first hour as the tablet disintegrates and a core of extended-release stimulant beads operating with a similar mechanism as those in Focalin XR.

So, how do these products compare to the original Concerta? We don’t know! Here are links to the FDA-required product information or “labels” for Concerta, the Mallinkcrodt generic version and the Kremers Urban generic version that are being substituted for Concerta. It appears that the FDA allowed the generic manufacturers to “cut and paste” the data from Concerta’s pharmacokinetic studies and clinical trials and present this information as if it represented trials each company conducted with their own unique product. It’s EXTREMELY UNLIKELY that different drug delivery systems would produce EXACTLY the same results in terms of drug metabolism (pharmacokinetics) and drug effects (pharmacodynamics) as the brand name drug.
The absorption of the original Concerta depends to some degree on an individual’s GI transit time…i.e., how long it takes for the pill to pass through the gut. Bead release systems (as in the Kremers Urban version) typically depend upon the acidity of the contents of the stomach at the time the extended-release bolus of medicine is needed. One would anticipate an individual child or teen might absorb significantly more (or less) medicine at different times during the day when two products that on average deliver roughly the same amount of medication over the same time period depend upon different physiologic processes.
When the FDA requires generic companies to do studies demonstrating “equivalency” to a brand medication, the amount of medication taken up into the body (measured by what we refer to as the “area under the curve” or AUC) is required to be within 80-125% of that observed with brand name drug. With some types of medication, that variability makes little difference. With stimulants, small differences in either the rate at which the medicine is absorbed or the time at which the medicine is absorbed make a PROFOUND difference in the benefits or side effects experienced by an individual child or adult. The FDA doesn’t require generic companies to conduct comparison studies showing that the products work as well in practice as the brand name drugs they’re intended to replace. Neither Mallinkcrodt nor Kremers Urban has been required by the FDA to conduct a study showing that their drug works as well in practice as the brand or authorized generic versions of Concerta.
Restating my earlier point, what makes Concerta work like Concerta is the OROS delivery system. The same drug (methylphenidate) released through a different delivery system produces a VERY different response.
In my mind, this is an utter and complete outrage when we’re talking about the most commonly prescribed drug for teenagers in the United States. I’d argue that this is a social justice issue. I’ve now had over ten kids come into my office for follow-up since the first of the year who have reported a significant decline in the effectiveness of their medication in the last couple of months. One nationwide drug store chain began ordering the Kudco product (the version many of my families have found to be less effective…the two main complaints being it doesn’t work as well or last as long as the original) in large quantities several months ago and substituting it for the authorized generic version of Concerta. What put me over the edge was an experience yesterday when I saw a mother and her daughter who reported problems with her medication since the appearance of her pill had changed. I sent them to the drugstore with new prescriptions for the brand Concerta or the authorized generic version. The mother was told by the pharmacy that it was illegal for them to fill the prescription for the original product even though she was willing to pay for the prescription “out of pocket” and that they would call the police if she insisted on having the prescription filled.
I’m at the end of my rope as a result of the administrative hassles involved with getting the kids in my practice the medications and educational support services they need to thrive in school, at home, with their friends and in community activities. I can’t even imagine what life must be like when parents have little money and need to depend upon our systems of care for support.
UPDATE #1: A small, randomized study has been published in Clinical Pediatrics demonstrating the superiority of the “brand” Concerta and generic Concerta using the OROS delivery system marketed by Actavis, compared to the Kudco and Mallinckrodt versions of generic Concerta using non-OROS delivery systems. Here’s the abstract:
Treatment effectiveness between equivalent doses of non-OROS (osmotic controlled release oral delivery system) methylphenidate ER and OROS methylphenidate ER (brand name Concerta) was examined in a clinical case series of children and adolescents followed for treatment of attention-deficit/hyperactivity disorder (ADHD). The Conners-Third Edition: Parent Rating Scale was used to compare ADHD symptoms when patients were taking non-OROS versus OROS at follow-up visits. A repeated-measures mixed-model approach was used to compare treatment effectiveness. The entire sample (N = 14) demonstrated a reduction in the mean score on the Inattention Scale from clinically significant (T-score > 65) to not clinically significant (T-score < 65) when patients were changed from non-OROS to OROS at the same dosage (mean T-score reduction = 23, p < .0001). The reduction in mean T-score after changing from non-OROS to OROS at the same dosage is indicative of improvement in symptoms of ADHD. Results provide empirical support for US Food and Drug Administration concerns regarding the therapeutic equivalence of non-OROS versus OROS for the treatment of ADHD.
UPDATE #2: The FDA did subsequently demand that each company submit additional data demonstrating their products to be equivalent to Concerta. Mallinckrodt did not comply with the request, while data submitted by Kremers Urban was deemed insufficient.
***********************************************************************************************************

Key Ministry has assembled a helpful resource page for church leaders and parents addressing the topic of ADHD and spiritual development. This page includes our blog series on the topic and links to helpful videos and resources for pastors, church staff, volunteers and parents. Access the resource page here.

